Surgical treatment of rectus femoris injuries in athletes
Lasse Lempainen
Hospital Mehiläinen NEO, Turku, Finland
Introduction
Rectus femoris muscle injuries are common in sports. Most of these injuries are strains or direct contusions which are treated by conservative means with good results. There are, however, also more severe rectus femoris injuries which can result in impaired athletic performance and long rehabilitation times. In these severe rectus femoris injuries surgical treatment can be also required.
Proximal ruptures
Proximal rectus femoris (PRF) ruptures are relatively rare injuries among top level athletes. PRF injuries can be complete avulsions or partial tears, and some of partial injuries seem have a tendency to progress to recurrent injuries.
Overall it seems that most of the injuries in the proximal insertional area are primarily suitable for conservative treatment and the outcome is mainly good. However, sometimes the healing does not progress as expected and return to play is delayed. This can occur in both complete and partial tears.
Operative treatment of complete PRF rupture has typically a good prognosis in professional soccer players. After suture anchor fixation of PRF rupture the athletes seem to return to the same level of competition with high probability. Figures 1-4 demonstrate complete proximal rectus femoris rupture causing clear retraction of the ruptured muscle belly.
Given the mainly good functional outcome and low complication rate, surgical treatment in proximal rectus femoris avulsions in professional soccer players is often recommended if conservative treatment does not yield in good results within a few months or if there is significant retraction of both tendon heads in a proximal avulsion. The full return to play can be even achieved after 3 to 4 months from the operation.
Mid-substance rectus femoris ruptures
The clinical entity considering mid-substance rectus femoris muscle ruptures is mainly lacking in the literature. These more serious mid-substance ruptures may cause significant functional loss in hip flexion and in knee extension strength, poor coordination as well as cramping pain and may require surgical intervention for proper healing.
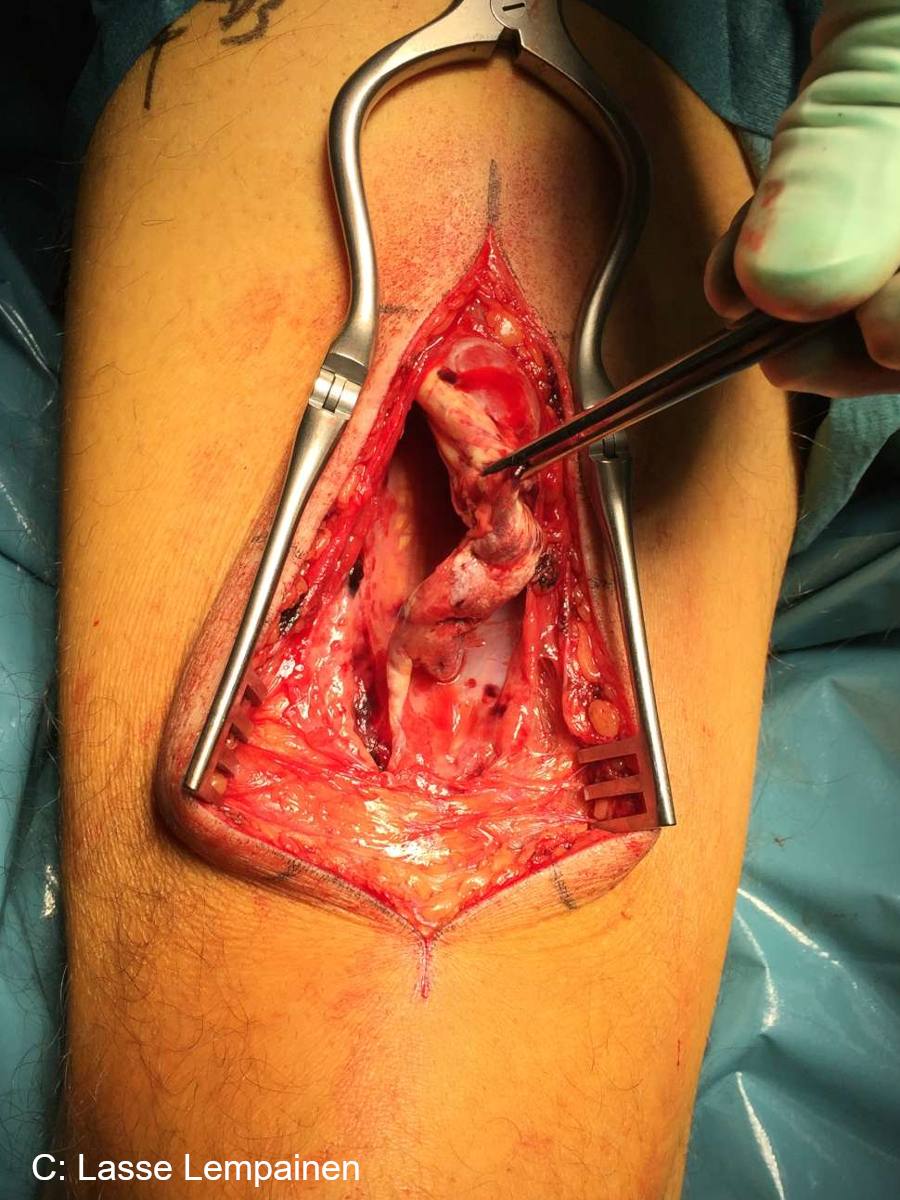
Based on my own experience, operative treatment for complete mid-substance rectus femoris rupture with clear cap between ruptured muscle ends is often beneficial for competitive athletes (Figures 5 and 6). Usually these athletes were able to return to their former level of sport after an average of 4-5 months from the surgery. If operation is done early after injury the anatomical repair can be done. In chronic phase fascia layers can be used to create bridge between ruptured ends (Figure 7).
Central tendon ruptures
Like in hamstring injuries rectus femoris injuries involving the central tendon seem to have a tendency to become chronic injuries. If central tendon is totally ruptured operative treatment may be the best option in top level athletes especially in recurrent injuries (Figures 8 and 9).
Quadriceps tendon ruptures
Complete and also severe partial quadriceps tendon ruptures should be operated acutely after injury (Figure 10).
In conclusion
There are many different types of tears that can occur in the rectus femoris muscle and the quadriceps muscle group. The indications for surgery are sometimes difficult to decide but chronic pain and disability that lasts for more than a few months after a complete or partial tear is definitely one of them. Surgery might also be considered in complete proximal avulsions with significant retraction or complete tears in which there is a significant gap between the tendon ends in the muscular part.
Literature:
Lempainen L, Kosola J, Pruna R, Puigdellivol J, Ranne J, Orava S. Operative Treatment of Proximal Rectus Femoris Injuries in Professional Soccer Players: A Series of 19 Cases. Orthop J Sports Med. 2018;6:2325967118798827.
Lempainen L, Kosola J, Niemi P, Orava S, Pruna R. Complete midsubstance rectus femoris ruptures: a series of 27 athletes treated operatively. Muscles Ligaments Tendons J. 2018;8:276-282.
-

- Figure 1. Proximal rectus femoris tendon rupture.

-

- Figure 2. Proximal rectus femoris tendon rupture.

-

- Figure 3. Proximal rectus femoris tendon rupture.

-

- Figure 4. Proximal rectus femoris tendon rupture.

-

- Figure 6. Acute complete mid-subtance rectus femoris rupture.

-

- Figure 6. Acute complete mid-subtance rectus femoris rupture.

-

- Figure 7. Chronic complete rectus femoris midsubstance rupture. Lack of tonus and scar tissue.

-

- Figure 5. Acute complete mid-subtance rectus femoris rupture.

-

- Figure 9. Central tendon rupture.
-

- Figure 10. Partial quadriceps tendon rupture (mri).




